Although it is one of the oldest paraclinic exams, dating back to the late 19th century, the ECG is still of crucial clinical use. This examination often still poses problems of interpretation to the medical practitioner.
This course aims to help the student, the practicing physician and even the trained cardiologist to improve his knowledge in electrocardiography. It consists of 250 traces of varying complexity with a description of each one by experts. This allows the reader to compare his analysis with that of the experts. In addition, the areas of interest of the ECG can be activated to be clearly highlighted.
We hope that these plots will be useful to readers and will improve their knowledge.
The ECGs are available sorted by keywords and categories.
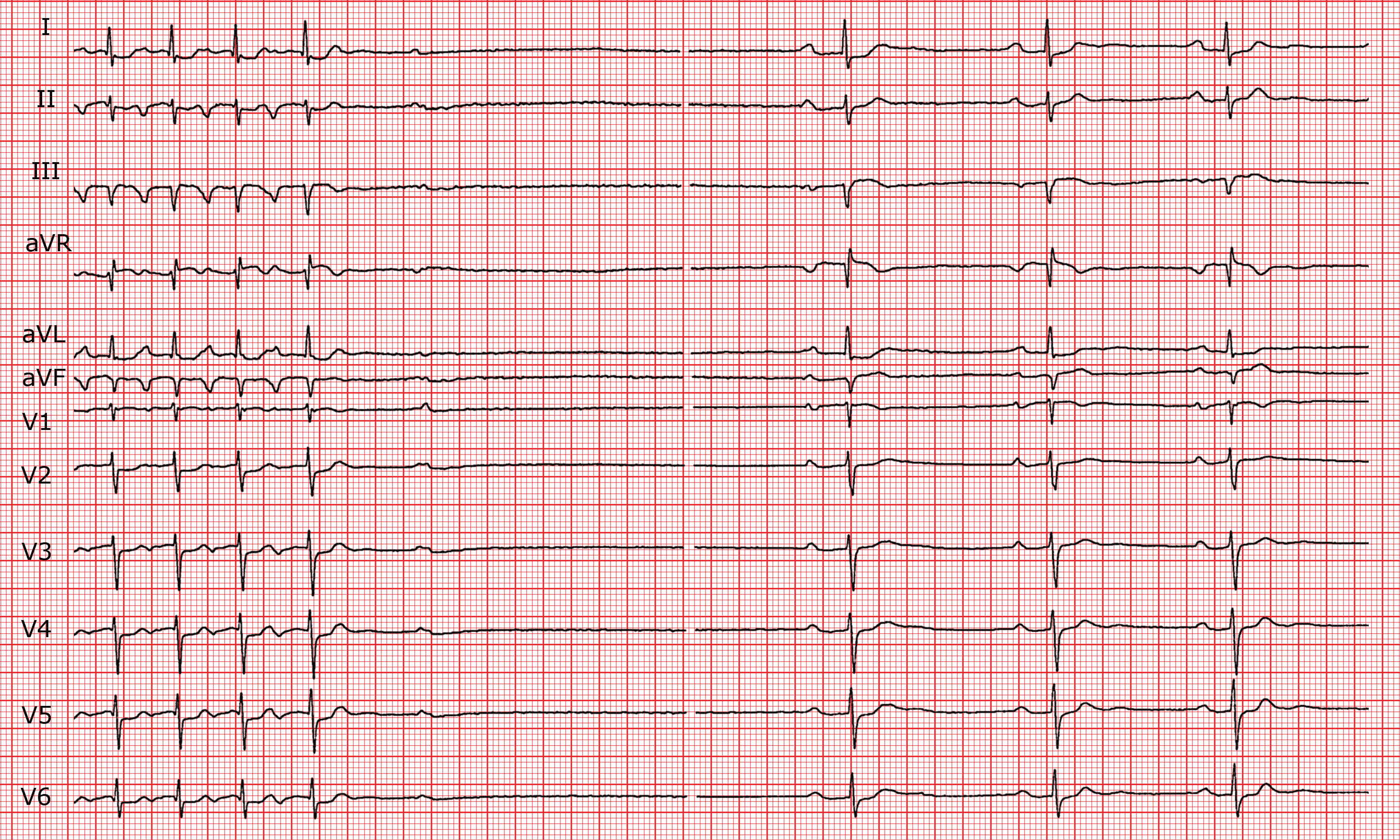
Sinus rhythm at 44 bpm. On the left side of the trace (first 7 complexes), narrow complex tachycardia; 135 bpm.
P waves
Normal in sinus rhythm, negative in II, III, aVF in tachycardia.
PR interval
Prolonged in sinus rhythm (260-320 ms); in tachycardia RP’>P’R interval.
QRS
Axis and morphology normal.
ST segment
Isoelectric.
T waves
Normal.
QT interval
Normal.
Zones
First degree A-V block.Interruption of the tachycardia without P' wave (retrograde block).Narrow QRS complexes tachycardia with RP' > P'R.
Diagnostic
Permanent junctional reciprocating tachycardia (Coumel's tachycardia or PJRT). First degree A-V block.
Comments
On the left side of the trace (first 7 complexes) narrow complex tachycardia can be seen. Each QRS complex is preceded by a P wave which is negative in II, III and aVF. Retrograde atrial activation is present. The RP'>P'R interval would suggest atrial tachycardia.
In the event of atrial tachycardia, carotid sinus massage provokes a transient A-V block with a series of blocked P waves. Here, the tachycardia stops over a QRS complex that is not followed by a P wave because it is interrupted by a conduction block in the retrograde pathway of a reentry circuit. Atypical atrioventricular nodal re-entrant tachycardia is a possible diagnosis but this is rare. PJRT or Coumel's tachycardia is the most probable diagnosis. Retrograde conduction occurs over an accessory pathway with slow conduction, which is shown by a relatively long RP' interval during the tachycardia. Coumel's tachycardia is a "permanent" tachycardia that usually occurs in young patients. Diagnosis is based for the large part on the patient's history.
During the post-tachycardia pause, after 800 ms, a blocked P wave occurs. Just under three seconds later sinus bradycardia with first degree A-Vblock is seen.