Although it is one of the oldest paraclinic exams, dating back to the late 19th century, the ECG is still of crucial clinical use. This examination often still poses problems of interpretation to the medical practitioner.
This course aims to help the student, the practicing physician and even the trained cardiologist to improve his knowledge in electrocardiography. It consists of 250 traces of varying complexity with a description of each one by experts. This allows the reader to compare his analysis with that of the experts. In addition, the areas of interest of the ECG can be activated to be clearly highlighted.
We hope that these plots will be useful to readers and will improve their knowledge.
The ECGs are available sorted by keywords and categories.
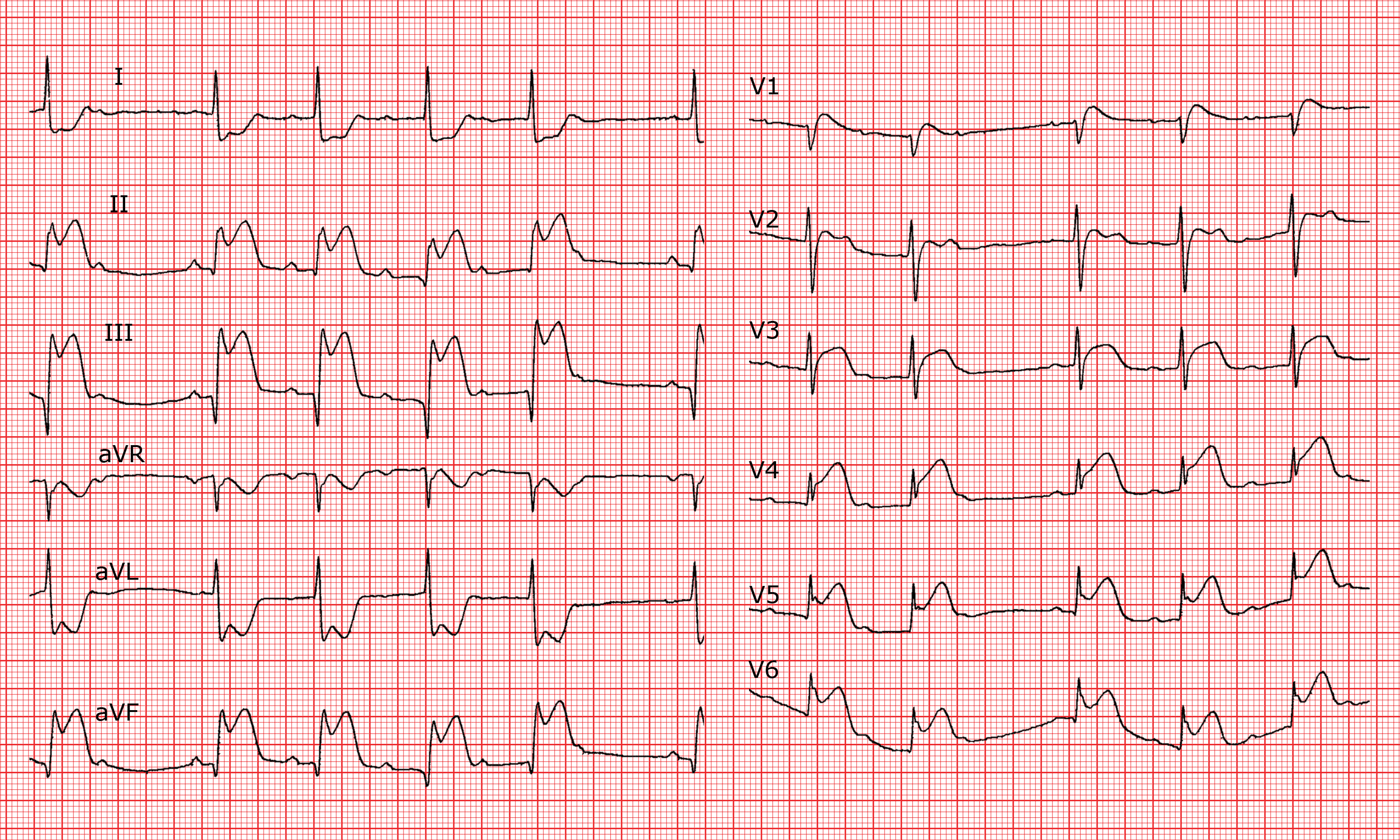
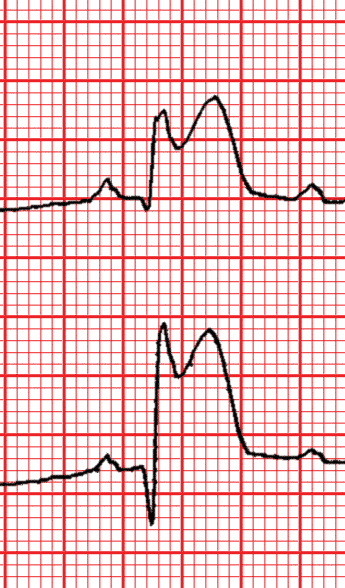
Prolonged duration in the leads with ST elevation, normal axis, Q waves in II, III, aVF.
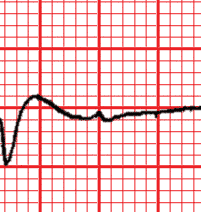
ST segment
Elevated in II, III and aVF, (with a mirror image depression in I, and aVL) and from V2 to V6.
T wave
Incorporated in the ST segment.
QT interval
Normal but at the upper limit of the normal range.
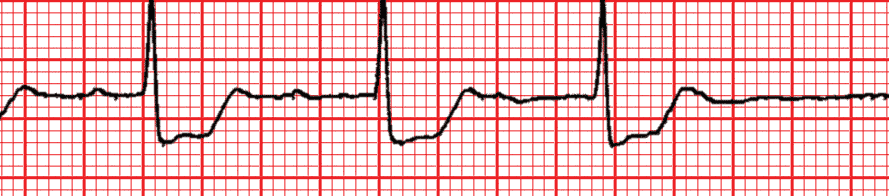
Zones
ST segment elevation in III > II.Blocked P wave.Progressive prolongation of the PR interval.
Diagnostic
Inferior myocardial infarction due to proximal occlusion of the right coronary artery, with second degree A-V block, Wenckebach type.
Comments
The ST elevation in II, III and aVF (with mirror images in I and aVL) indicates inferior myocardial infarction. More marked in III than in II, it allows the occlusion to be located in the right coronary artery. The A-V conduction disturbance confirms that the lesion is also in the artery of the A-V node, which is a branch of the right coronary artery located relatively near the origin of the right coronary artery. Occlusion is therefore proximal, as confirmed by the ST elevation over all the percordial leads. The localisation diagnosis could be verified in a right precordial lead (V4R), which should record an ST elevation > 1mm, preceding a positive T wave. Elevation in the precordial leads indicates an anterior ischaemic lesion. This type of A-V block is generally reversible and, provided that it is asymptomatic, does not require implantation of a temporary pace maker.